

What Baton Rouge Clinics Can Learn From Better Exam-Room Cleaning Workflows
For outpatient clinics, exam-room cleaning is often treated as a necessary routine rather than a strategic operating system. Yet in high-turnover medical environments, that distinction matters. A room reset is not simply the end of one patient encounter. It is the beginning of the next one, and the quality of that transition shapes infection-control consistency, staff coordination, patient trust, and day-to-day reliability. In Baton Rouge, where outpatient care continues to carry a large share of the region’s clinical activity, better exam-room cleaning workflows offer a useful lesson. They show that cleaning is far more effective when treated as a repeatable process rather than a general expectation.
Why Outpatient Clinics Need More Than General Cleaning Expectations
Many clinics assume they have a workable cleaning system because staff members understand that rooms must be cleaned between patients. The problem is that general awareness is not the same as a controlled workflow. Without a defined sequence, a room-turnover process can vary depending on who is on shift, how busy the clinic feels, where supplies are positioned, and what interruptions occur during the reset. That kind of variation is common in outpatient care because staff members are constantly balancing competing priorities. The issue is not usually a lack of effort. It is that effort alone that does not guarantee consistency.
Better workflows solve that problem by replacing broad assumptions with a more structured method. They clarify what gets cleaned, in what order, and according to what standard. They reduce the need for improvisation when volume increases. They also make performance easier to teach, observe, and reinforce. In practical terms, a stronger workflow turns room turnover from a memory-based task into an operational routine that can be maintained under pressure.
Infection-Control Consistency Depends on Repeatability
In exam rooms, repeatability matters because the environment contains the same categories of high-touch surfaces and patient-contact areas repeatedly. When the cleaning process varies, even slightly, the clinic introduces unevenness into a function that should be tightly controlled. One room may get a thorough reset. Another may look just as clean but reflect a different sequence or a missed touchpoint. Over time, those differences create a system that feels acceptable on the surface but becomes less reliable beneath the surface.
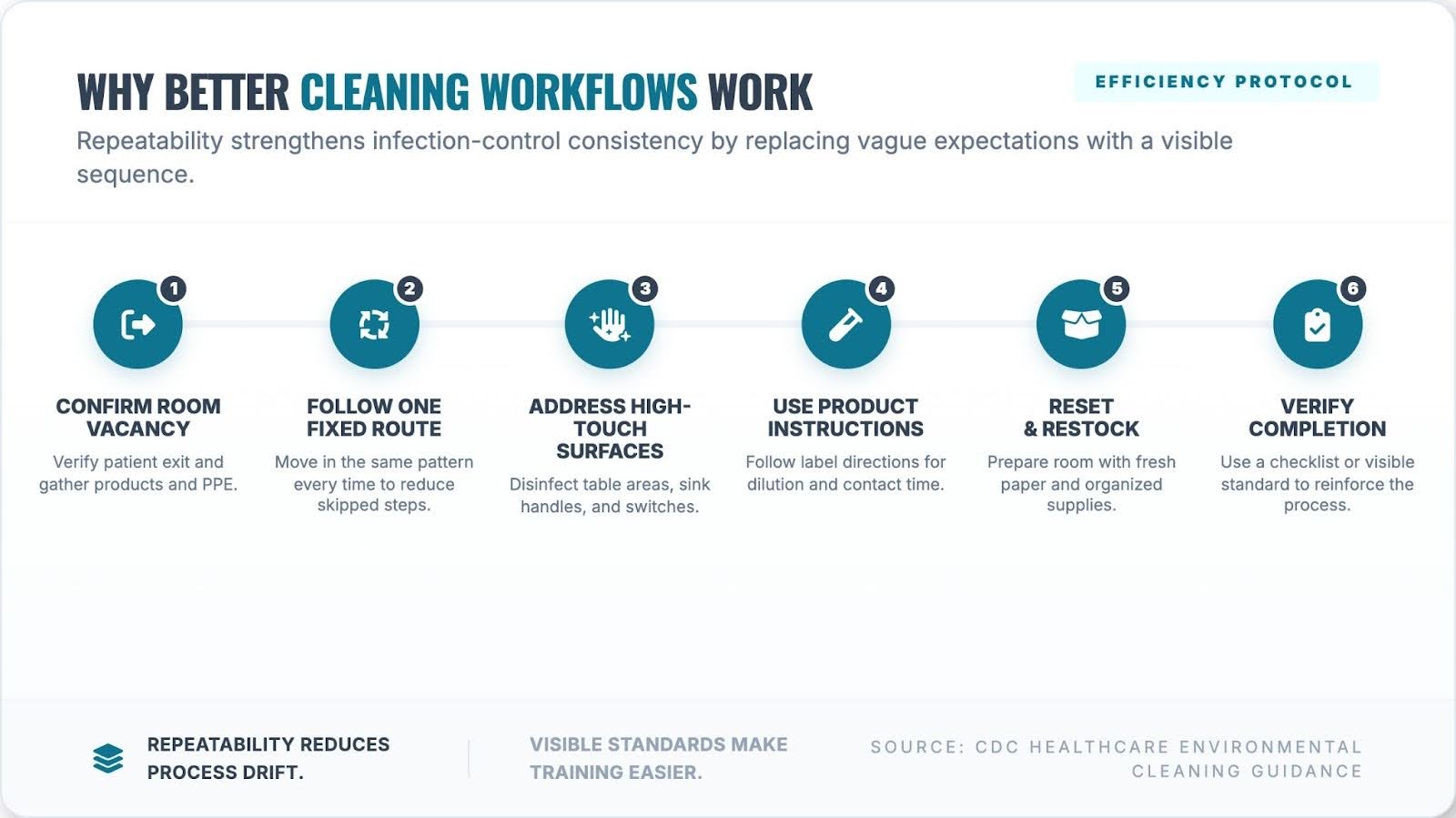
The CDC’s guidance on healthcare cleaning procedures emphasizes systematic methods, defined cleaning processes, and consistent attention to high-touch patient-care surfaces. That guidance matters for outpatient clinics because it reinforces a simple principle. Cleaning is not strongest when it is merely well-intended. It is strongest when it is standardized. In fast-moving clinical settings, repeatability is what allows infection-control expectations to survive a busy day.
The Baton Rouge Example Highlights a Broader Outpatient Reality
A recent Baton Rouge-focused article, Why Infection-Control Consistency Is Becoming a Bigger Urgent Care Issue in Baton Rouge, framed this challenge through the lens of urgent care operations. Its larger lesson extends well beyond urgent care. The article argued that room turnover should not be judged solely by how quickly it occurs, but by whether it is structured enough to remain consistent across rooms, shifts, and staff members. That is a useful takeaway for Baton Rouge clinics more broadly, because many outpatient settings face the same operational pressures, even if their patient flow differs from that of urgent care on the surface.

Specialty clinics, walk-in settings, and general outpatient practices all rely on controlled environments that must be reset reliably throughout the day. They may have different visit patterns, but they still depend on the same underlying discipline. A room that is turned over inconsistently introduces uncertainty into the patient environment. A room reset through a stable workflow supports smoother operations and greater confidence in the facility’s standards. The local lesson, then, is not limited to one type of clinic. It is relevant anywhere repeated room use intersects with infection-prevention expectations.
Workflow Discipline Helps Clinics Manage Volume Without Drift
One of the clearest advantages of a better exam-room cleaning workflow is that it reduces drift during busy periods. In most clinics, the problem is not the first room turnover of the day. It is the tenth, the twentieth, or the one that happens while the front desk is busy, a provider needs support, and a patient is already waiting for the next room. Under those conditions, staff members are more likely to compress steps, change sequence, or rely on visual shortcuts. That is where a defined workflow becomes valuable. It protects quality by giving employees a pattern that holds up when the clinic becomes harder to manage.
Workflow discipline also reduces ambiguity. Staff members no longer have to decide in real time what “clean enough” means in a particular moment. The process itself answers that question. That matters because ambiguity is often where inconsistency begins. When a task has a clear sequence and a visible endpoint, it becomes easier to perform it well under ordinary operational stress. For managers, that also means stronger supervision. It is much easier to reinforce a known process than to evaluate an informal one that changes according to habit.
Training and Auditing Become Easier With Defined Procedures
Better workflows also improve the clinic’s ability to train staff members and maintain accountability. New employees learn faster when expectations are concrete rather than implied. Experienced staff members are less likely to drift into personal shortcuts when the room-turnover routine is clearly defined. Supervisors gain a more stable basis for coaching because they can evaluate whether the sequence was followed, rather than relying solely on whether the room appears presentable.
The CDC’s outpatient infection-prevention guide supports this kind of operational discipline by emphasizing written procedures, staff training, and consistent implementation in outpatient settings. Those recommendations are especially relevant for clinics that want to strengthen audit readiness and reduce the risk of process variation over time. A site that can describe its exam-room workflow in clear terms is in a stronger position than one that depends on broad verbal expectations. Defined procedures make the cleaning program more visible, more teachable, and more defensible.
Patients Experience Workflow Quality Even if They Never See the Checklist
Clinics sometimes view room turnover as a purely internal process, but patients experience its effects firsthand. They may not know the exact sequence used between visits, yet they quickly notice whether a room feels orderly, reset, and prepared. That perception has operational value because outpatient care depends heavily on trust. In many cases, patients do not have a long-standing relationship with every clinic they enter. They form impressions quickly, and the physical environment becomes part of how they judge the site’s professionalism.
A better exam-room cleaning workflow helps support that confidence because consistency tends to show. A stable process produces a room that feels controlled rather than hurried. It reinforces the sense that the clinic is managing the environment with intention rather than simply reacting to pressure. In Baton Rouge, where clinics compete not only on medical services but also on convenience and patient experience, that kind of visible operational discipline matters more than it may at first appear.
Why Baton Rouge Clinics Should Treat Cleaning Workflow as an Operations Issue
The strongest lesson from better exam-room cleaning workflows is that they belong inside the broader operations conversation. Cleaning is not separate from throughput, staff coordination, or patient confidence. It influences all three. When workflows are weak, variation enters quietly and becomes harder to correct. When workflows are strong, clinics gain a more reliable system for maintaining room readiness, ensuring infection-control consistency, and preserving the overall feel of the facility.
For Baton Rouge clinics, that lesson is especially relevant because outpatient care environments are being asked to manage volume without sacrificing professionalism or control. Better workflows help them do that by creating a room-turnover process that is less dependent on circumstances and more dependent on structure. In a busy outpatient setting, that difference can shape how well the clinic performs over time.
Conclusion
What Baton Rouge clinics can learn from better exam-room cleaning workflows is simple but important. Cleaning works best when it is not treated as a vague expectation or a hurried afterthought. It works best when it is organized, repeatable, and built into the facility’s operating rhythm. That kind of structure supports consistent infection control, better staff alignment, stronger oversight, and a more trustworthy patient environment. In outpatient care, the room reset is not just a maintenance task. It is one of the clearest tests of whether the clinic’s workflow can remain consistent when the day becomes demanding.
{kind=link}